
Experimental and Molecular Medicine, 10/06/2026
Introduction
Osteoarthritis (OA) affects more than 600 million people and is a leading cause of disability, with a rising prevalence driven by aging and obesity. Current treatments (NSAIDs, corticosteroids, HA, PRP, BMAC) primarily provide temporary symptom relief and do not modify disease progression; repeated corticosteroid use may even induce chondrotoxicity. Consequently, a treatment gap exists for patients with moderate disease—who are not yet candidates for joint replacement but lack effective long-term options. This has driven demand for disease-modifying therapies.
Cell therapy, particularly mesenchymal stem cells (MSCs), has emerged as a promising approach due to its multimodal mechanisms, including immunomodulation, macrophage polarization, chondroprotection, and support for tissue regeneration. However, superior clinical benefits compared with existing therapies have not yet been clearly demonstrated.
Although hundreds of cell therapy products are currently in development, the transition rate from early- to late-phase trials remains low, and no products have been approved in the United States, the European Union, or the United Kingdom for OA. This review focuses on evaluating the biological rationale, clinical evidence, regulatory frameworks, and operational challenges of MSC-based therapies in the treatment of OA.

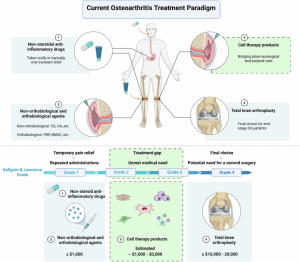
Fig. 1: Current osteoarthritis treatment paradigm. (1) non-steroidal anti-inflammatory drugs administered orally or topically during the early stages of OA; (2) non-orthobiological intra-articular injections such as corticosteroids (CSs) or hyaluronic acid (HA), and orthobiological injections including platelet-rich plasma (PRP) or bone marrow aspirate concentrate (BMAC), also primarily used in early stages of OA; (3) prospective cell therapy products, mainly delivered through intra-articular injection, intended to bridge the therapeutic gap between early-stage and late-stage OA; (4) total knee arthroplasty as the final intervention when disease progression continues despite the aforementioned treatments.
Regulatory expectations for cell therapy products
Regulatory requirements in Europe and the United States are increasingly focused on: viability assays; the correlation between viable cell counts and clinical efficacy; defined minimum thresholds for cell viability; tight control ranges for total cell numbers and viable cell counts; the impact of non-viable cells (e.g., immunogenicity); long-term safety follow-up (2–5 years); local administration with systemic monitoring; cell persistence versus transient effects (e.g., M2 macrophage polarization and stromal activation); and cellular safety (e.g., risks of tumorigenicity, viral contamination, or microbial contamination during culture).
Emerging directions in cell therapy product development
- Advances in manufacturing operations (room-temperature stability and compliance with Good Manufacturing Practice – GMP).
- Stratification of mesenchymal stem cell (MSC) potency according to patient phenotypes (“MSC matching/compatibility”) through cell-based assays.
- Development of novel vector technologies to enhance safety, achieve higher efficacy, enable non-integration, and prolong therapeutic effects in genetically modified cell therapy products.
- A shift toward truly regenerative approaches, utilizing advanced bioengineered scaffolds in combination with genetically modified cell therapies.
- Movement toward cell-free therapies based on the secretome and extracellular vesicles.
Biology of cell therapy products in OA
Recent evidence suggests that the therapeutic activity of cell therapy products in OA depends less on their direct differentiation into chondrocytes and is primarily mediated through paracrine and immunomodulatory mechanisms. For example, MSCs secrete a wide range of cytokines, growth factors, and extracellular vesicles (EVs) capable of modulating the joint microenvironment.
Notably, senescent chondrocytes and MSCs within the OA joint contribute to disease progression through the senescence-associated secretory phenotype (SASP), which promotes inflammation and matrix degradation. Preclinical data indicate that MSCs derived from young, healthy sources, when administered intra-articularly, can counteract these processes, whereas senescent MSCs exhibit limited therapeutic efficacy, highlighting the importance of cell source for potency and proliferative capacity. Accordingly, allogeneic MSCs from young, healthy donors may have theoretical or preclinical advantages over autologous MSCs derived from aged patients; however, this advantage has not yet been confirmed in head-to-head clinical trials.
Chondrocytes and genetically modified packaging cells
Chondrocytes maintain the extracellular matrix (ECM) of articular cartilage; however, in OA they undergo phenotypic changes (hypertrophy, senescence) and increase the secretion of catabolic enzymes (MMPs, ADAMTS), thereby promoting cartilage degeneration.
Chondrocyte-based therapies face several limitations, including low proliferative capacity, the risk of dedifferentiation during culture, and strong dependence on the microenvironment, thus requiring appropriate scaffolds. Consequently, they are less developed in OA compared with MSCs. However, the role of dedifferentiation remains unclear, as paracrine mechanisms may be more important than direct cell replacement.
Some promising “off-the-shelf” approaches include chondrocytes derived from polydactyly (with strong proliferative capacity and stable phenotype) and nasal chondrocytes (robust ECM production, already applied clinically). In addition, combinatorial strategies using chondrocytes with genetically modified cells (e.g., HEK-293 cells expressing TGF-β1) are being investigated to enhance therapeutic efficacy.

Fig. 2: Current cell sources for clinical osteoarthritis cell therapy products.
Mesenchymal stem cells
MSCs have been studied since the 1960s and continue to attract significant interest in clinical trials. Although they have the capacity to differentiate into chondrocyte-like cells (as observed in early-stage OA studies), their primary mechanism of action is not direct cell replacement. Despite low survival rates in the inflammatory environment of OA, MSCs can still modulate disease progression through multimodal mechanisms of action.
MSCs can be derived from multiple sources: adult tissues (adipose tissue, bone marrow, dental tissue) and perinatal tissues (placenta, umbilical cord blood, Wharton’s jelly). A major limitation of expanded MSCs is their tendency toward hypertrophic differentiation. MSCs derived from bone marrow, adipose tissue, umbilical cord, placenta, amniotic fluid, and induced pluripotent stem cells (iPSCs) are being developed into cell therapy products for OA treatment.
The emergence of allogeneic, “off-the-shelf” MSC products aims to reduce variability and enable large-scale, standardized manufacturing for broader application. In contrast, autologous MSC therapies (post-expansion), although safer in terms of immune compatibility, are labor-intensive, time-consuming, highly variable between batches, and the most costly. iPSC-based therapies (studied since 2006) represent a promising direction but still face multiple translational barriers, including lack of standardization, predictability, reproducibility, and regulatory challenges.
Therapeutic mechanism of action
The therapeutic effects of MSCs can be categorized into several major mechanistic groups as follows:
Immunomodulation and paracrine signalling
MSCs exert their effects primarily through the secretome, particularly extracellular vesicles (EVs). EVs contain miRNAs, lncRNAs, and immunoregulatory proteins that help protect the joint by promoting chondrocyte proliferation, reducing apoptosis, increasing ECM gene expression, inhibiting catabolic enzymes, activating autophagy, and reducing ferroptosis. Therefore, cell-free approaches (exosomes/secretome) are being considered promising strategies.
The core mechanism of MSCs is immunomodulation: reducing pro-inflammatory factors (TNF-α, IL-1β, IL-6, MMPs, ADAMTS), while promoting macrophage polarization from M1 to M2 in the synovium. This creates an anti-inflammatory environment with increased IL-4, IL-10, and TGF-β. In addition, MSCs secrete IL-1Ra, which helps block inflammatory signaling via IL-1.
Chondroprotective and neuromodulatory effects
MSCs contribute to cartilage protection by reducing chondrocyte apoptosis, enhancing ECM synthesis, limiting hypertrophy, and attenuating the senescence-associated phenotype (SASP). A novel mechanism is mitochondrial transfer from MSCs to chondrocytes, which helps reduce oxidative stress and improve cellular metabolism. In addition, MSCs inhibit the transition toward a fibroblast-like phenotype, thereby limiting fibrosis.
Regarding pain relief, direct evidence remains limited; however, MSCs may exert effects through multiple mechanisms: interaction with pain mediators (such as substance P and CGRP) and indirect analgesic effects via reduction of synovial inflammation (decreasing TNF-α, IL-1β, IL-6, and increasing anti-inflammatory factors).
Other cell sources
Fibroblasts can be isolated from various tissues, as they are the primary cell type responsible for extracellular matrix (ECM) production. In OA treatment, multipotent fibroblasts have been modified and derived from gingival tissue. Gingiva-derived fibroblasts are proposed to possess immunomodulatory properties and multimodal activity similar to MSCs.
Peripheral blood mononuclear cells (PBMCs) can be obtained from circulating blood through centrifugation and lymphocyte layer separation. In OA therapeutic applications, allogeneic PBMCs have been cultured, irradiated, and cryopreserved. They are proposed to have the ability to modulate immune responses within the osteoarthritic knee joint.
Current clinical development landscape
Most clinical trials of cell therapy for OA use VAS (pain), WOMAC/IKDC (function), and KOOS, along with MRI imaging assessments. However, there is no direct clinical evidence demonstrating mechanisms such as macrophage polarization, cytokine reduction, or secretome effects within the human joint; these mechanisms are primarily based on in vitro studies and animal models, and thus have not been definitively validated in humans.
Sustained efficacy is often explained by the “hit-and-run” model, in which the short-term action of administered cells triggers long-lasting biological responses (immunomodulation, tissue reprogramming, endogenous repair, and pain relief). However, these mechanisms have not been directly confirmed in humans, and confounding factors such as natural fluctuation and placebo effects should be considered. Adverse events are typically mild and transient (pain, swelling at the injection site), while serious events are rare and mostly associated with underlying comorbidities.
Prominent clinical programs
Among approximately 40 clinical candidates for OA, six programs stand out; five involve intra-articular injection and one requires a surgical procedure.
Cartistem (Medipost): Human umbilical cord blood–derived MSCs, implanted via arthrotomy with subchondral drilling and 4% HA. Targets severe OA (ICRS 3–4). Long-term follow-up studies show improvements in VAS, IKDC, WOMAC, and ICRS scores up to 3–5 years, with no serious adverse events reported. Advancing toward trials in the United States.
Stempeucel (Stempeutics): Allogeneic, pooled bone marrow–derived MSCs, administered via intra-articular injection at 25 million cells + HA, targeting KL grade 2–3. Phase II showed safety but no superiority over HA; Phase III reported improvements in WOMAC and MRI with no disease progression. Approved in India.
Progenza (Regeneus): Allogeneic adipose-derived MSCs for KL grade 1–3. Phase I showed improvements in VAS and WOMAC at 3–12 months, with relatively low cell doses compared to other products.
TG-C (Kolon TissueGene): The only genetically modified cell therapy currently in development for OA (KL 2–3). Comprises chondrocytes plus genetically modified GP2-293 cells expressing TGF-β1, administered via intra-articular injection. A large Phase III trial (~530 patients) is ongoing; preclinical models demonstrate analgesic and immunomodulatory effects.
Allocetra (Enlivex): An allogeneic PBMC-based “apoptosis-induced” therapy, administered intra-articularly for KL grade 2–3. Its mechanism is based on immunomodulation through macrophage interaction; safety has been demonstrated in Phase I/II studies.
PLX-PAD (Pluri Biotech): Allogeneic MSC-like cells derived from placenta, administered intra-articularly. Demonstrated safety in Phase III trials for other indications; currently in Phase I/IIa trials for OA. The primary mechanism involves secretion of cytokines, chemokines, and growth factors to modulate immune responses and reduce inflammation.
Practical and operational challenges
- Manufacturing and standardization: GMP processes are complex; differences in cell sources (bone marrow, adipose tissue, umbilical cord) and culture techniques introduce significant product-to-product variability, affecting reproducibility.
- Supply chain challenges: Strict cold-chain requirements, time control, and maintenance of cell viability pose barriers to implementation.
- Logistical challenges: A short “use window” (48–72 hours, practically 24–48 hours post-shipment) complicates treatment scheduling.
- Comparison with orthobiologics: Cell therapies must demonstrate onset within 2–6 weeks, efficacy lasting ≥6 months, improvements in imaging, delay of surgery, and biomarker changes—yet standardized biomarkers are still lacking.
Future directions and scientific gaps
- Clinical value: Primarily depends on durability of efficacy and cost. Benefits should be sustained for ≥12 months (preferably longer) to compete with CS, HA, and PRP.
• Key endpoints: Ability to delay surgery/TKA. Trials should be large-scale with 2–5 years of follow-up, focusing on time to surgery/TKA alongside VAS/NRS and WOMAC.
• Biological strategies: Enhancing durability using scaffolds, hydrogels, and microcarrier systems to improve cell survival and paracrine effects; however, clinical evidence remains limited. Cell-free approaches (EVs) may reduce cost and logistical burden.
• Gaps: Lack of standardized assays for MSCs (viable cell count, immunogenicity, secretome), creating challenges for reproducibility and regulatory control.
→ Future success will depend more on long-term evidence and economic viability than on mechanistic complexity.
Conclusions
Cell therapy for OA is a promising therapeutic approach but remains insufficiently validated, particularly in KL grade 2–3. Early data show improvements in pain and function; however, clinical implementation is still limited by complex manufacturing, regulatory barriers, and high costs.
The key determinant is durability of efficacy and the ability to slow disease progression (delay surgical indication and TKA). Without demonstrating sustained and disease-modifying benefits, these therapies are unlikely to outperform simpler options such as PRP, HA, or other autologous products. Biologically, MSCs and related platforms exhibit immunomodulatory and regenerative mechanisms, but the OA joint environment constrains their long-term effectiveness. Emerging approaches such as scaffolds, EVs, and gene therapies may enhance efficacy, yet robust clinical evidence is still lacking.
In summary, the future of cell therapy depends on demonstrating durable, reproducible, and disease-modifying effects in OA; otherwise, it will remain a high-cost adjunctive option.
References
Lili Cui, Ming Xiao, Qian Zhang, Haijie Liu, Yi Ren, Gaoting Ma, Da Zhou, Qingfeng eitso, V., Ellis, R., Ng, K. et al (2026). Next-generation therapies for osteoarthritis: the evolving role of cell therapy products. Exp Mol Med.
Source: Experimental and Molecular Medicine.



