


Cell Reports Medicine, 28/05/2026
Introduction
Stroke is a leading cause of mortality and disability; among them, ischemic stroke accounts for the majority and is expected to continue increasing. Current treatments remain limited due to the narrow reperfusion window, and rehabilitation is the main option in the later stage; therefore, new strategies are needed to improve neurological deficits.
Cell therapy, particularly mesenchymal stem cells (MSCs), has shown efficacy in animal models through mechanisms such as immunomodulation, neuroprotection, promotion of angiogenesis, and reconstruction of neural networks. However, clinical evidence remains inconsistent and the optimal strategy has not been determined. MSCs have advantages including ease of acquisition, low immunogenicity, and fewer ethical concerns; they can be derived from bone marrow, adipose tissue, and umbilical cord. MSCs from perinatal tissues (such as the umbilical cord) have superior biological potential, but have been less studied clinically compared to other sources.
Most trials have focused on the acute or chronic phases, while the subacute phase (particularly 3–6 months, when recovery reaches a plateau) represents a potential window for intervention. The optimal route of administration remains unclear, but intravenous delivery is commonly used due to its safety and minimal invasiveness. This phase 1 study evaluates the safety of allogeneic UC-MSCs administered intravenously in patients with subacute stroke (18 patients, 3 dose levels). Results: no serious adverse events were observed; one case of seizure may be related. Functional improvement was noted, but caution is needed due to the open-label, single-arm design.
Methods
Study design
Phase 1, open-label, single-arm, single-center, dose-escalation study (50, 100, 200 million UC-MSCs).
- Sample size: 18 patients (12 males, 6 females; mean age 52.5 ± 9.0), divided into 3 dose groups (6 patients per group).
- Follow-up: 24 weeks to assess safety and tolerability.
- DLT: adverse events ≥ grade 3 (CTCAE v5.0), possibly related to treatment, within 28 days post-infusion.
- Toxicity threshold: <33%; dose escalation allowed only when <2/6 patients at the previous dose level experience DLT.
- Ethics: approved by the Ethics Committee (code [2022]043), conducted in accordance with the Declaration of Helsinki; all patients/legal representatives provided written informed consent.
Participants
Inclusion criteria:
- Age 18–80.
- Anterior circulation ischemic stroke, confirmed by CT/MRI, occurring 12–24 weeks prior to enrollment.
- NIHSS score 6–20, with NIHSS 1a < 2.
Exclusion criteria:
- History of other neurological/psychiatric disorders (intracranial hemorrhage, brain tumor, Parkinson’s disease, severe depression, etc.).
- Severe diseases of the cardiovascular, respiratory, renal, hepatic, or immune systems.
- Inability to undergo MRI.
MSC transplantation
Procedures ensured sterility, cell quality, and dose control prior to infusion.
Pre-infusion preparation:
- Cells were automatically thawed and suspended in 50 mL of 0.9% NaCl + 0.25% human albumin under sterile conditions.
- Viability >90% (assessed by AO-DAPI staining).
Dose groups: Three dose levels: 50, 100, 200 million UC-MSCs, with 6 patients per group.
Administration:
- Single intravenous infusion within 2 hours after preparation.
- Infusion rate 1–2 mL/min, using a blood transfusion set with a 170 μm filter.
Endpoints
Primary endpoint: Assessment of safety and tolerability of UC-MSCs over 24 weeks, based on:
- Adverse events (AEs) and serious adverse events (SAEs)
- Laboratory tests (complete blood count, biochemistry, etc.)
- Other assessments such as electrocardiogram
→ AEs were classified and graded according to CTCAE v5.0, and their relationship to treatment was evaluated.
Secondary endpoints: Preliminary efficacy assessed by changes from baseline at weeks 12 and 24:
- Scales: mRS, BI, NIHSS, Fugl-Meyer (FM)
- Infarct volume
- Proportion of patients achieving BI ≥ 95 (mRS: 0 = no symptoms, 6 = death; higher scores = worse outcomes)
Exploratory endpoint: Changes in peripheral immunity after UC-MSC treatment.
Imaging: Brain MRI was performed at baseline (pre-treatment) and at 4, 12, and 24 weeks after UC-MSC infusion.
Immunological tests
- Objective: to evaluate changes in peripheral immunity before and after UC-MSC treatment.
• Cytokine quantification (12 types): IL-1β, IL-2, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12P70, IL-17, IFN-α, IFN-γ, TNF-α.
Results
Patient characteristics
Phase 1, open-label, single-arm, single-center study (NCT05697718). Among 128 patients with ischemic stroke screened, 22 were assessed as eligible; inclusion criteria included: age 18–80, anterior circulation stroke confirmed by CT/MRI 12–24 weeks prior to enrollment, NIHSS score 6–20, and item 1a <2.
A total of 18 patients (12 males, 6 females; mean age 52.5 ± 9.0) were enrolled from April 2023 to January 2024. All received a single intravenous infusion of UC-MSCs at escalating doses of 50, 100, or 200 million cells (n = 6 per group). At baseline (12–24 weeks post-stroke), patients had a median mRS of 4.5 (IQR 4–5) and a median NIHSS of 9 (IQR 8–12). The mean time from stroke onset to cell infusion was 122.2 ± 22.7 days.

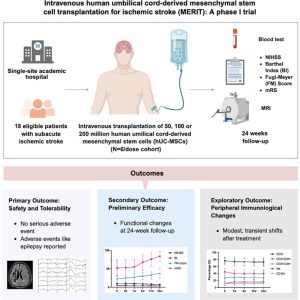
Figure 1. The diagram of the study procedure. After assessment of eligibility, the patients received cell infusion. They were followed up for 24 weeks and observed for tolerance. Clinical scoring, blood tests, and MRI were performed before and after cell infusion. Some icons of the figure were created with BioRender. UC-MSCs.
Primary outcome: Safety and tolerability
All patients were followed for 24 weeks to assess the safety and tolerability of UC-MSCs (primary endpoint). Dose-limiting toxicity (DLT) was defined as any adverse event (AE) of grade ≥3 according to CTCAE v5.0 with at least a possible relationship to treatment.
A total of 48 AEs were recorded (30 grade 1, 18 grade 2); all patients recovered spontaneously or after short-term intervention. No serious adverse events (SAEs) or DLTs were observed following UC-MSC infusion. Reported AEs included pain/swelling in the paretic limb, elevated ALT, falls, hypoglycemia, constipation, etc.; most were assessed as unrelated or unlikely related to treatment.
Two patients experienced 5 AEs considered possibly related to treatment:
- One patient developed transient infusion-related symptoms (dizziness, nausea, sweating, fatigue), occurring near the end of infusion and resolving spontaneously after ~10 minutes.
- Another patient (with prior right hemispheric cortical infarction 103 days earlier) developed a generalized tonic–clonic seizure 1 day after infusion of 200 million UC-MSCs; treated with intramuscular phenobarbital and oral levetiracetam. The patient had two additional similar episodes on days 81 and 140 post-infusion. Due to temporal association, the event was conservatively classified as “possibly related,” although cortical infarction is a known risk factor for post-stroke epilepsy.
Regarding laboratory findings: no significant changes were observed in hematology (except for a decrease in monocyte percentage at week 12), and no changes in coagulation function. Some patients showed mild, transient increases in D-dimer after infusion without symptoms or evidence of thrombosis. Total protein and albumin levels increased significantly (persisting to week 24). No clinically significant changes were observed in liver or renal function, blood glucose, uric acid, or lipid profiles; ECG, brain MRI, and clinical examinations revealed no notable abnormalities after treatment.
Secondary outcome: Preliminary efficacy
Secondary endpoints included functional assessments (mRS, BI, NIHSS, Fugl-Meyer) and infarct volume at 12 and 24 weeks post-infusion compared with baseline; the proportion of patients achieving BI ≥95 was also recorded. All patients completed 12-week follow-up, and 16/18 completed 24 weeks.
Results showed functional improvement over time:
- mRS decreased by ~0.9 points (12 weeks, 14/18 patients) and ~1.0 point (24 weeks, 13/16).
- NIHSS decreased by 1.6 points (12 weeks) and 2.4 points (24 weeks).
• Fugl-Meyer increased by 10.5 points (12 weeks) and 14.7 points (24 weeks).
• BI increased by 23.9 points (12 weeks) and 31.6 points (24 weeks); 3/18 patients achieved BI ≥95 at 12 weeks and 5/16 at 24 weeks.
No significant differences were observed between dose levels, and no time–dose interaction was detected.
Infarct volume was measured by an independent, blinded assessor using ITK-SNAP software on MRI FLAIR images. Compared with baseline, infarct volume showed a slight, non-significant increase at 12 weeks (+0.5 ± 3.7 mL) and a slight decrease at 24 weeks (−1.4 ± 7.1 mL), with no statistical significance.
Post hoc exploratory analysis by baseline infarct size (≤50 mL vs. >50 mL) suggested that patients with smaller infarcts tended to have greater volume reduction, but no difference in functional improvement was observed.
Exploratory outcome: Peripheral immunological changes after treatment
Peripheral lymphocyte subsets and circulating inflammatory mediators were assessed to investigate immune changes following UC-MSC infusion. Flow cytometry analysis showed mild, transient alterations in immune cell composition: decreased proportions of CD3+, CD4+ T cells, CD19+ B cells, and the CD4/CD8 ratio; along with increased CD8+ T cells and NK cells. These changes were more pronounced in the early post-infusion phase, but no statistically significant differences were observed across time points or dose levels.
Quantitative analysis of plasma cytokines showed a slight trend toward decreased pro-inflammatory cytokines (IL-5, IL-1β, IL-17A) and increased anti-inflammatory cytokines (IL-4, IL-10) after treatment. Complement components (C3, C4) and immunoglobulins (IgA, IgG, IgM) increased slightly, while CRP tended to decrease.
Post hoc correlation analysis showed that changes in IL-4 and IL-10 were positively correlated with improvement in Fugl-Meyer scores at 24 weeks; conversely, changes in immunoglobulins (IgA, IgG, IgE) were negatively correlated with functional improvement.
Discussion
This phase 1 trial provides preliminary evidence that intravenous infusion of cryopreserved allogeneic UC-MSCs in patients with subacute ischemic stroke is safe and well tolerated. No SAEs or DLTs were observed; adverse events were infrequent, mostly mild, and transient.
Infusion-related adverse effects included dizziness, nausea, sweating, and fatigue—consistent with previous studies. No embolic events were observed; although mild transient increases in D-dimer occurred, there were no clinical manifestations. Instant blood-mediated inflammatory reaction (IBMIR) may occur but appeared limited with moderate doses and low-passage cells.
A notable safety concern is post-infusion seizure: one case was reported, possibly treatment-related but with underlying risk factors (large cortical infarction). The seizure incidence was not higher than in non–cell-treated patients, but careful monitoring is still required. Tumorigenic risk remains unclear, warranting long-term follow-up (up to 30 years).
Regarding efficacy, functional improvements (mRS, NIHSS, FM, BI) were observed in many patients; however, these cannot be conclusively attributed to treatment due to the lack of a control group and potential influence of spontaneous recovery and rehabilitation. No significant changes in infarct volume were observed, and no clear dose–response relationship was identified.
Immunological analyses showed mild, transient changes, suggesting immunomodulatory effects of MSCs. Some immune markers correlated with functional improvement, but these findings are exploratory and do not establish causality.
Conclusion, intravenous UC-MSC infusion is feasible and demonstrates preliminary safety across three dose levels. Signals of efficacy and immunological effects are suggestive and require confirmation in larger, randomized controlled trials.
Limitations of the study
- Small sample size and lack of a control group → difficult to confirm efficacy.
- Open-label design and non-standardized treatment → prone to confounding (spontaneous recovery, rehabilitation).
- Optimal dose not determined; high inter-patient variability.
- Limited follow-up and imaging endpoints, with minimal changes observed.
- Immunological analyses are exploratory and do not establish causality.
→ Efficacy findings are only suggestive and require confirmation in large-scale randomized controlled trials (RCTs).
References
Lili Cui, Ming Xiao, Qian Zhang, Haijie Liu, Yi Ren, Gaoting Ma, Da Zhou, Qingfeng Ma, Hui Yao, Ming Lin, Daiquan Gao, Linlin Ye, Ran Wang, Yelin Wang, Lan Zhang, Lianmei Zhong, Ge Gao, Jieli Chen, Jukka Jolkkonen, Johannes Boltze, Junwei Hao (2026). Intravenous human umbilical cord-derived mesenchymal stem cell transplantation for ischemic stroke (MERIT): A phase 1 trial. Cell Reports Medicine, 102836.
Source: Cell Reports Medicine
Link: https://www.cell.com/cell-reports-medicine/fulltext/S2666-3791(26)00253-3



